What Is Causing Bunions To Appear?
Overview
 A bunion occurs when the big to begins to deviate towards the second toe. The biggest misconception is that bunions occur from an overgrowth of bone. While this may be true in very few people, the bunion really represents a dislocation or subluxation of the big toe joint and it bulges against the skin. This bony prominence is what is commonly called a bunion. Sometimes the bunion area may become irritated, red and/or callused.
A bunion occurs when the big to begins to deviate towards the second toe. The biggest misconception is that bunions occur from an overgrowth of bone. While this may be true in very few people, the bunion really represents a dislocation or subluxation of the big toe joint and it bulges against the skin. This bony prominence is what is commonly called a bunion. Sometimes the bunion area may become irritated, red and/or callused.
Causes
Bunions are most often caused by an faulty foot mechanics. It is not the bunion itself that is inherited, but certain foot types that make a person prone to developing a bunion. Although wearing shoes that crowd the toes won't actually cause bunions in the first place, it sometimes makes the deformity get progressively worse. That means you may experience symptoms sooner.
Symptoms
The symptoms of a bunion include the following development of a firm bump on the outside edge of the foot, at the base of the big toe, redness, swelling, or pain at or near the MTP joint, corns or other irritations caused by the overlap of the first and second toes, restricted or painful motion of the big toe.
Diagnosis
Your doctor is very likely to be able to diagnose your bunion simply by examining your foot. Even before that, he or she will probably ask about your family and personal medical history and evaluate the types of shoes you wear. You'll be asked about your symptoms, when they started and when they occur. You may also be asked to flex your toe so that your doctor can get an idea of your range of motion. He or she may order x-rays in order to determine the extent of your deformity.
Non Surgical Treatment
The initial treatment of a bunion should be non-operative. Symptoms can often be greatly improved with simple non-operative interventions. Non-operative treatment may include properly fitted shoes, Properly fitting comfort shoes with a wide non-constrictive toe box, especially one that is made out of a soft material such as leather, can be quite helpful in reducing the irritation over the prominent bunion. In some instances, it is helpful to have a shoemaker stretch the inside aspect of the shoe. Jamming a foot with a bunion into a constrictive shoe will likely lead to the development of uncomfortable symptoms. Bunion pads, Medial bunion pads may also be helpful in decreasing the symptoms associated with the bunion. These pads can be obtained at many drugstores. Essentially, they serve to lessen the irritation over the medial prominence and, thereby, decrease the associated inflammation This should be combined with comfortable non-constrictive shoes. A toe spacer placed between the great toe and the second toe can help to reduce the bunion deformity and, thereby, decrease the stretch on the medial tissue and the irritation associated with the bunion. Toe spacers can be obtained at most drug stores or online. Soft shoe inserts. Over-the-counter accommodative orthotics may also help bunion symptoms. This product is particularly helpful if bunion symptoms include pain that is under the ball of the foot. Orthotics with a slight medial longitudinal arch may be helpful for patients that have associated flatfoot deformity. These can be purchased at many sports stores, outdoors stores, or pharmacies. Bunion splints have often been used to treat the symptoms associated with hallux valgus. These splints are typically worn at night in an effort to reduce the bunion deformity. There is no evidence to suggest that these splints decrease the rate at which bunion deformities occur. There is also no evidence that clearly supports their effectiveness. However, some patients report good relief with the use of these splints.
Will Overpronation Involve An Operation
Overview
Your feet are the foundation for your entire body. When this foundation is misaligned or functioning poorly the effects can be felt throughout the body, whether in muscle and joint pain or through more serious injuries. Over 75% of the population suffers from overpronation or excessive supination, yet most of us are unaware of our own foot type and how it affects the rest of our body.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
If ignored, overpronation can lead to complications such as hammer toes, corns and calluses, shin splints, hallux rigidus and many more foot and lower leg problems. Hammer toes appear when the toes are placed under too much pressure and the ligaments and muscles in the toes begin to reduce in size, leading to the curvature of the toes and making them look like little hammers. Overpronators can develop hammertoes if they don?t wear an appropriate pair of shoes. Corns and calluses also appear as a result of overpronation. They form in response to excess pressure, and overpronators may find that they have excessive hard skin on the balls of the feet and inside edge of the big toe. It is the body?s way of protecting against excessive forces and friction. They can be painful.
Diagnosis
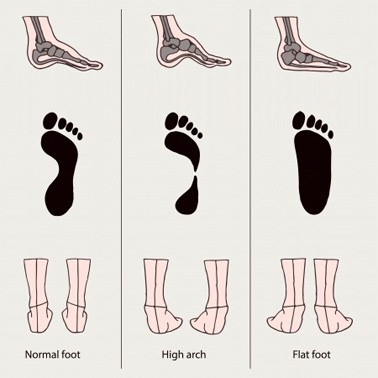
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Your feet are the foundation for your entire body. When this foundation is misaligned or functioning poorly the effects can be felt throughout the body, whether in muscle and joint pain or through more serious injuries. Over 75% of the population suffers from overpronation or excessive supination, yet most of us are unaware of our own foot type and how it affects the rest of our body.
Causes
Overpronation often occurs in people with flat feet, whose plantar fascia ligament is too flexible or too long, and therefore unable to properly support the longitudinal arch of the foot. People tend to inherit the foot structure that leads to overpronation. In a normal foot the bones are arranged so that two arches are formed, the longitudinal and the transverse. Ligaments hold all the bones in their correct positions, and tendons attach muscles to bones. If the bones are held together too loosely, they will tend to move inwards as this is the easiest direction for them to go. Over time the soft tissue structures will adjust to the misalignment and the foot will become permanently over-flexible, with a flat arch.
Symptoms
If ignored, overpronation can lead to complications such as hammer toes, corns and calluses, shin splints, hallux rigidus and many more foot and lower leg problems. Hammer toes appear when the toes are placed under too much pressure and the ligaments and muscles in the toes begin to reduce in size, leading to the curvature of the toes and making them look like little hammers. Overpronators can develop hammertoes if they don?t wear an appropriate pair of shoes. Corns and calluses also appear as a result of overpronation. They form in response to excess pressure, and overpronators may find that they have excessive hard skin on the balls of the feet and inside edge of the big toe. It is the body?s way of protecting against excessive forces and friction. They can be painful.
Diagnosis
Firstly, look at your feet in standing, have you got a clear arch on the inside of the foot? If there is not an arch and the innermost part of the sole touches the floor, then your feet are over-pronated. Secondly, look at your running shoes. If they are worn on the inside of the sole in particular, then pronation may be a problem for you. Thirdly, try the wet foot test. Wet your feet and walk along a section of paving and look at the footprints you leave. A normal foot will leave a print of the heel, connected to the forefoot by a strip approximately half the width of the foot on the outside of the sole. If you?re feet are pronated there may be little distinction between the rear and forefoot, shown opposite. The best way to determine if you over pronate is to visit a podiatrist or similar who can do a full gait analysis on a treadmill or using forceplates measuring exactly the forces and angles of the foot whilst running. It is not only the amount of over pronation which is important but the timing of it during the gait cycle as well that needs to be assessed.
Non Surgical Treatment
The following exercises help retrain the foot and ankle complex to correct overpronation. Exercises may be performed while wearing shoes, or for an even greater challenge, in bare feet. Duck Stand. This exercise is designed to prepare for the more dynamic BT exercises ahead by waking up the gluteal muscles and teaching clients how the gluteal muscles control the degree of foot pronation. For example, when the glutes contract concentrically, they rotate the leg outward. As the leg rotates outward, the arch of the foot raises (i.e., supinates). Stand beside the BT with both heels together and feet turned outward. (Note: As you progress, perform this exercise while standing on the BT.) Try to rotate legs outward by tightening buttock muscles while tilting pelvis under. As legs rotate outward, arches of the feet raise up out of pronation. Hold position for 30 seconds. Big Toe Pushdowns. This exercise is designed to strengthen the muscle of the big toe that holds up the arch of the foot (i.e., flexor hallucis longus muscle). This stops the foot from overpronating. Stand on top of the BT dome with feet facing forward. Use gluteal muscles to raise the arches of the feet (see previous exercise - "Duck Stand"). Keep arches raised while pushing down big toe into the BT. While pushing down, tension build in the arch on the underside of their foot should be felt. Hold position for 15 seconds.
Surgical Treatment
Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults.
An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer.
Severs Disease Facts And Figures
Overview
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
There are several theories as to the cause of this condition. These range from a tight Achilles tendon, to micro stress fractures of the calcaneal apopyhsis. The prevailing theory suggests that the condition occurs when the child's growth plate is at its weakest. Combined with increased athletic activity, improper shoe gear and trauma the heel becomes inflamed and painful.
Symptoms
Unilateral or bilateral heel pain. Heel pain during physical exercise, especially activities that require running or jumping or are high impact. Pain is often worse after exercise. A tender swelling or bulge on the heel that is painful on touch. Limping. Calf muscle stiffness first thing in the morning.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Depending on the Podiatrist's diagnosis and the severity of the pain, there are several treatment options available. Rest/ reduced activity: your child should reduce or stop any activity that causes pain, such as sports and running. This can be a difficult option, as children are normally quite willful in pursuit of their favorite pastimes! Over the counter anti-inflammatory drugs, such as ibuprofen (found in Nurofen), to help reduce pain and inflammation. Try to make sure your child does the recommended stretching exercises before sport/play. This will should help reduce the stress on the fascia tendon and relieve heel pain. The use of Orthotic insoles. Footactive Kids orthotics are made for children. They will help properly support the foot, help prevent over-pronation or improper gait restoring your child's foot the the correct biomechanical position. If you are in any doubt or your child's foot pain persists then please arrange an appointment with a Podiatrist or Physiotherapist. Please click here for more information on the use of orthotics for children.
Recovery
It may take several weeks or months for the pain to completely stop. When the pain is completely gone, your child may slowly return to his or her previous level of activity.
When recurring heel pain occurs in children, it is usually due to Sever's Disease, while adult heel pain is usually due to heel spurs, plantar fasciitis, or retrocalcaneal bursitis (Haglund's Deformity). Calcaneus is the anatomical name of the heel bone. Sever's Disease or Calcaneal Apophysitis is an inflammation of the growth plate located at the posterior aspect (back) of the heel.
Causes
There are several theories as to the cause of this condition. These range from a tight Achilles tendon, to micro stress fractures of the calcaneal apopyhsis. The prevailing theory suggests that the condition occurs when the child's growth plate is at its weakest. Combined with increased athletic activity, improper shoe gear and trauma the heel becomes inflamed and painful.
Symptoms
Unilateral or bilateral heel pain. Heel pain during physical exercise, especially activities that require running or jumping or are high impact. Pain is often worse after exercise. A tender swelling or bulge on the heel that is painful on touch. Limping. Calf muscle stiffness first thing in the morning.
Diagnosis
You may have pain when your doctor squeezes your heel bone. You may have pain when asked to stand or walk on your toes or on your heels. You may have pain in your heel when your doctor stretches your calf muscles. Your doctor may order x-rays of the injured foot to show an active growth plate.
Non Surgical Treatment
Depending on the Podiatrist's diagnosis and the severity of the pain, there are several treatment options available. Rest/ reduced activity: your child should reduce or stop any activity that causes pain, such as sports and running. This can be a difficult option, as children are normally quite willful in pursuit of their favorite pastimes! Over the counter anti-inflammatory drugs, such as ibuprofen (found in Nurofen), to help reduce pain and inflammation. Try to make sure your child does the recommended stretching exercises before sport/play. This will should help reduce the stress on the fascia tendon and relieve heel pain. The use of Orthotic insoles. Footactive Kids orthotics are made for children. They will help properly support the foot, help prevent over-pronation or improper gait restoring your child's foot the the correct biomechanical position. If you are in any doubt or your child's foot pain persists then please arrange an appointment with a Podiatrist or Physiotherapist. Please click here for more information on the use of orthotics for children.
Recovery
It may take several weeks or months for the pain to completely stop. When the pain is completely gone, your child may slowly return to his or her previous level of activity.
The Causes And Treatment
Overview
Adult Acquired Flatfoot (Posterior Tibial Tendon Dysfunction) is a painful, progressive deformity in adults. It results from a gradual stretch (attenuation) of the tibialis posterior tendon and the ligaments that support your foot?s arch. This stretching causes the tendon to lose strength and function. Many people have flat feet and do not experience pain. However, pain occurs with Adult Acquired Flatfoot because the tendons and ligaments have been torn. Once the vital ligaments and posterior tibial tendon are lost, there is no longer anything holding the arch of the foot in place. 
Causes
Women are affected by Adult Acquired Flatfoot four times more frequently than men. Adult Flatfoot generally occurs in middle to older age people. Most people who acquire the condition already have flat feet. One arch begins to flatten more, then pain and swelling develop on the inside of the ankle. This condition generally affects only one foot. It is unclear why women are affected more often than men. But factors that may increase your risk of Adult Flatfoot include diabetes, hypertension, and obesity.
Symptoms
Often, this condition is only present in one foot, but it can affect both. Adult acquired flatfoot symptoms vary, but can swelling of the foot's inner side and aching heel and arch pain. Some patients experience no pain, but others may experience severe pain. Symptoms may increase during long periods of standing, resulting in fatigue. Symptoms may change over time as the condition worsens. The pain may move to the foot's outer side, and some patients may develop arthritis in the ankle and foot.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Conservative (nonoperative) care is advised at first. A simple modification to your shoe may be all that???s needed. Sometimes purchasing shoes with a good arch support is sufficient. For other patients, an off-the-shelf (prefabricated) shoe insert works well. The orthotic is designed specifically to position your foot in good alignment. Like the shoe insert, the orthotic fits inside the shoe. These work well for mild deformity or symptoms. Over-the-counter pain relievers or antiinflammatory drugs such as ibuprofen may be helpful. If symptoms are very severe, a removable boot or cast may be used to rest, support, and stabilize the foot and ankle while still allowing function. Patients with longer duration of symptoms or greater deformity may need a customized brace. The brace provides support and limits ankle motion. After several months, the brace is replaced with a foot orthotic. A physical therapy program of exercise to stretch and strengthen the foot and leg muscles is important. The therapist will also show you how to improve motor control and proprioception (joint sense of position). These added features help prevent and reduce injuries. 
Surgical Treatment
Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss.
The Facts About Adult Aquired FlatFoot
Overview
Adult acquired flatfoot is a progressive disorder that involves a compromise of soft tissue supports of the medial arch. The condition most commonly affects middle aged women and is characterized by lowering of the arch, turning out of the forefoot, and a sideways angulation of the heel. There are five stages of the disorder that becomes progressively disabling. The end stage can potentially compromise the ankle joint along with the joints in the hindfoot.
Causes
Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
It is imperative that you seek treatment should you notice any symptoms of a falling arch or PTTD. Due to the progressive nature of this condition, your foot will have a much higher chance of staying strong and healthy with early treatment. When pain first appears, your doctor will evaluate your foot to confirm a flatfoot diagnosis and begin an appropriate treatment plan. This may involve rest, anti-inflammatory medications, shoe modifications, physical therapy, orthotics and a possible boot or brace. When treatment can be applied at the beginning, symptoms can most often be resolved without the need for surgery.
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
Adult acquired flatfoot is a progressive disorder that involves a compromise of soft tissue supports of the medial arch. The condition most commonly affects middle aged women and is characterized by lowering of the arch, turning out of the forefoot, and a sideways angulation of the heel. There are five stages of the disorder that becomes progressively disabling. The end stage can potentially compromise the ankle joint along with the joints in the hindfoot.
Causes
Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors.
Symptoms
Patients often experience pain and/or deformity at the ankle or hindfoot. When the posterior tibial tendon does not work properly, a number of changes can occur to the foot and ankle. In the earlier stages, symptoms often include pain and tenderness along the posterior tibial tendon behind the inside of the ankle. As the tendon progressively fails, deformity of the foot and ankle may occur. This deformity can include progressive flattening of the arch, shifting of the heel so that it no longer is aligned underneath the rest of the leg, rotation and deformity of the forefoot, tightening of the heel cord, development of arthritis, and deformity of the ankle joint. At certain stages of this disorder, pain may shift from the inside to the outside aspect of the ankle as the heel shifts outward and structures are pinched laterally.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
It is imperative that you seek treatment should you notice any symptoms of a falling arch or PTTD. Due to the progressive nature of this condition, your foot will have a much higher chance of staying strong and healthy with early treatment. When pain first appears, your doctor will evaluate your foot to confirm a flatfoot diagnosis and begin an appropriate treatment plan. This may involve rest, anti-inflammatory medications, shoe modifications, physical therapy, orthotics and a possible boot or brace. When treatment can be applied at the beginning, symptoms can most often be resolved without the need for surgery.
Surgical Treatment
For patients with a more severe deformity, or significant symptoms that do not respond to conservative treatment, surgery may be necessary. There are several procedures available depending on the nature of your condition. Ligament and muscle lengthening, removal of inflamed tendon lining, transferring of a nearby tendon to re-establish an arch, and bone realignment and fusion are examples of surgical options to help with a painful flatfoot condition. Surgery can be avoided when symptoms are addressed early. If you are feeling ankle pain or notice any warmth, redness or swelling in your foot, contact us immediately. We can create a tailored treatment plan to resolve your symptoms and prevent future problems.
What Is The Main Cause Of Achilles Tendinitis ?
Overview
 The Achilles tendon attaches your calf muscles to your heel. You use this tendon to jump, walk, run, and stand on the balls of your feet. Continuous, intense physical activity, like running and jumping, can cause inflammation of the Achilles. This is known as Achilles tendonitis (also spelled tendinitis). Achilles tendonitis can often be treated at home using simple strategies. However, if home treatment doesn?t work, it is important to see a doctor. If your tendonitis gets worse, it can lead to a tendon tear. You may need medication to ease the pain or a surgical repair.
The Achilles tendon attaches your calf muscles to your heel. You use this tendon to jump, walk, run, and stand on the balls of your feet. Continuous, intense physical activity, like running and jumping, can cause inflammation of the Achilles. This is known as Achilles tendonitis (also spelled tendinitis). Achilles tendonitis can often be treated at home using simple strategies. However, if home treatment doesn?t work, it is important to see a doctor. If your tendonitis gets worse, it can lead to a tendon tear. You may need medication to ease the pain or a surgical repair.
Causes
Excessive exercise is a common cause of Achilles tendonitis. This is particularly true for athletes. However, factors unrelated to exercise may also contribute to risk. Rheumatoid arthritis and infection are both correlated with tendonitis. In general, any repeated activity that strains the Achilles tendon can contribute to this problem. Here are a few possible causes, jumping into an exercise routine without a proper warm-up, straining calf muscles during repeated exercise or physical activity, playing sports such as tennis that require quick stops and changes of direction, wearing old or ill-fitting shoes, wearing high heels every day.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Nonsurgical methods include rest and stop doing activities that cause stress to the tendon. Ice the area by applying ice to the tendon for 15 minutes after exercising. Compress the tendon by using an athletic wrap or surgical tape. Elevate your injury. You can reduce swelling by lying down and raising your foot at a level that is above your heart. Stretch your ankles and calf muscles. Take anti-inflammatory medication (e.g.: ibuprofen to reduce swelling). Wear orthotics and running shoes. Take part in physical therapy.

Surgical Treatment
In cases of severe, long-term Achilles tendonitis the sheath may become thick and fibrous. In these cases surgery may be recommended. Surgery aims to remove the fibrous tissue and repair any tears in the tendon. A cast or splint will be required after the operation and a recovery program including physiotherapy, specific exercises and a gradual return to activity will be planned.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
The Achilles tendon attaches your calf muscles to your heel. You use this tendon to jump, walk, run, and stand on the balls of your feet. Continuous, intense physical activity, like running and jumping, can cause inflammation of the Achilles. This is known as Achilles tendonitis (also spelled tendinitis). Achilles tendonitis can often be treated at home using simple strategies. However, if home treatment doesn?t work, it is important to see a doctor. If your tendonitis gets worse, it can lead to a tendon tear. You may need medication to ease the pain or a surgical repair.
Causes
Excessive exercise is a common cause of Achilles tendonitis. This is particularly true for athletes. However, factors unrelated to exercise may also contribute to risk. Rheumatoid arthritis and infection are both correlated with tendonitis. In general, any repeated activity that strains the Achilles tendon can contribute to this problem. Here are a few possible causes, jumping into an exercise routine without a proper warm-up, straining calf muscles during repeated exercise or physical activity, playing sports such as tennis that require quick stops and changes of direction, wearing old or ill-fitting shoes, wearing high heels every day.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
During an examination of the foot and ankle, you doctor will look for the following signs, Achilles tendon swelling or thickening. Bone spurs appearing at the lower part of the tendon at the back of the hell. Pain at the middle or lower area of the Achilles tendon. Limited range of motion of the foot and ankle, and a decreased ability to flex the foot. Your doctor may perform imaging tests, such as X-rays and MRI scans, to make a diagnosis of Achilles tendinitis. X-rays show images of the bones and can help the physician to determine if the Achilles tendon has become hardened, which indicated insertional Achilles tendinitis. MRI scans may not be necessary, but they are important guides if you are recommended to have surgical treatment. An MRI can show the severity of the damage and determine what kind of procedure would be best to address the condition.
Nonsurgical Treatment
Nonsurgical methods include rest and stop doing activities that cause stress to the tendon. Ice the area by applying ice to the tendon for 15 minutes after exercising. Compress the tendon by using an athletic wrap or surgical tape. Elevate your injury. You can reduce swelling by lying down and raising your foot at a level that is above your heart. Stretch your ankles and calf muscles. Take anti-inflammatory medication (e.g.: ibuprofen to reduce swelling). Wear orthotics and running shoes. Take part in physical therapy.
Surgical Treatment
In cases of severe, long-term Achilles tendonitis the sheath may become thick and fibrous. In these cases surgery may be recommended. Surgery aims to remove the fibrous tissue and repair any tears in the tendon. A cast or splint will be required after the operation and a recovery program including physiotherapy, specific exercises and a gradual return to activity will be planned.
Prevention
To prevent Achilles tendonitis or tendonosis from recurring after surgical or non-surgical treatment, the foot and ankle surgeon may recommend strengthening and stretching of the calf muscles through daily exercises. Wearing proper shoes for the foot type and activity is also important in preventing recurrence of the condition.
What Is Pain On The Heel And The Best Ways To Remedy It

Overview
Plantar fasciitis is a poorly understood condition. There is little consensus among medical professionals about what causes the problem, and no treatments have been reliably proven to treat it. A number of theories exists for why plantar fasciitis develops, but the ineffectiveness of conventional treatments suggests something is missing. The plantar fascia is a band of connective tissue that runs along the underside of the foot from the heel to the toes. The fascia helps maintain the integrity of the arch, provides shock absorption, and plays an important role in the normal mechanical function of the foot.
Causes
Plantar fasciitis occurs when the thick band of tissue on the bottom of the foot is overstretched or overused. This can be painful and make walking more difficult. You are more likely to get plantar fasciitis if you Have foot arch problems (both flat feet and high arches), run long distances, downhill or on uneven surfaces, are obese or gain weight suddenly, have a tight Achilles tendon (the tendon connecting the calf muscles to the heel), wear shoes with poor arch support or soft soles. Plantar fasciitis is seen in both men and women. However, it most often affects active men ages 40 - 70. It is one of the most common orthopedic foot complaints. Plantar fasciitis was commonly thought to be caused by a heel spur. However, research has found that this is not the case. On x-ray, heel spurs are seen in people with and without plantar fasciitis.
Symptoms
Among the symptoms for Plantar Fasciitis is pain usually felt on the underside of the heel, often most intense with the first steps after getting out of bed in the morning. It is commonly associated with long periods of weight bearing or sudden changes in weight bearing or activity. Plantar Fasciitis also called “policeman’s heel” is presented by a sharp stabbing pain at the bottom or front of the heel bone. In most cases, heel pain is more severe following periods of inactivity when getting up and then subsides, turning into a dull ache.
Diagnosis
A physical exam performed in the office along with the diagnostic studies as an x-ray. An MRI may also be required to rule out a stress fracture, or a tear of the plantar fascia. These are conditions that do not normally respond to common plantar fasciitis treatment.
Non Surgical Treatment
The plantar fascia is a band of tissue, much like a tendon, that starts at your heel and goes along the bottom of your foot. It attaches to each one of the bones that form the ball of your foot. The plantar fascia works like a rubber band between the heel and the ball of your foot to form the arch of your foot. If the band is short, you'll have a high arch, and if it's long, you'll have a low arch, what some people call flatfeet. A pad of fat in your heel covers the plantar fascia to help absorb the shock of walking. Damage to the plantar fascia can be a cause of heel pain.

Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints, a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as, open surgery, where the section of the plantar fascia is released by making a cut into your heel, endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to, have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Stretching Exercises
Exercises designed to stretch both your calf muscles and your plantar fascia (the band of tissue that runs under the sole of your foot) should help relieve pain and improve flexibility in the affected foot. A number of stretching exercises are described below. It's usually recommended that you do the exercises on both legs, even if only one of your heels is affected by pain. This will improve your balance and stability, and help relieve heel pain. Towel stretches. Keep a long towel beside your bed. Before you get out of bed in the morning, loop the towel around your foot and use it to pull your toes towards your body, while keeping your knee straight. Repeat three times on each foot. Wall stretches. Place both hands on a wall at shoulder height, with one of your feet in front of the other. The front foot should be about 30cm (12 inches) away from the wall. With your front knee bent and your back leg straight, lean towards the wall until you feel a tightening in the calf muscles of your back leg. Then relax. Repeat this exercise 10 times before switching legs and repeating the cycle. You should practise wall stretches twice a day. Stair stretches. Stand on a step of your stairs facing upstairs, using your banister for support. Your feet should be slightly apart, with your heels hanging off the back of the step. Lower your heels until you feel a tightening in your calves. Hold this position for about 40 seconds, before raising your heels back to the starting position. Repeat this procedure six times, at least twice a day. Chair stretches. Sit on a chair, with your knees bent at right angles. Turn your feet sideways so your heels are touching and your toes are pointing in opposite directions. Lift the toes of the affected foot upwards, while keeping the heel firmly on the floor. You should feel your calf muscles and Achilles tendon (the band of tissue that connects your heel bone to your calf muscle) tighten. Hold this position for several seconds and then relax. Repeat this procedure 10 times, five to six times a day. Dynamic stretches. While seated, roll the arch of your foot (the curved bottom part of the foot between your toes and heel) over a round object, such as a rolling pin, tennis ball or drinks can. Some people find that using a chilled can from their fridge has the added benefit of helping to relieve pain. Move your foot and ankle in all directions over the object for several minutes. Repeat the exercise twice a day.